
Manori Prasadani Thambiliyagodage1*, Arjuna Salinda Athapathu1, Surantha Perera2
1post graduate institute of Medicine, Colombo, Sri Lanka.
2Castle street Hospital for Women, Colombo, Sri Lanka.
*Corresponding Author: Manori Prasadani Thambiliyagodage, post graduate institute of Medicine, Colombo, Sri Lanka.
Received: April 21, 2022
Accepted: May 04, 2022
Published: May 10, 2022
Citation: Manori Prasadani Thambiliyagodage, Arjuna Salinda Athapathu, Surantha Perera (2022). “Stridor with Respiratory Distress as an Immediate Presentation of Arnold Chiari Malformation - A Rare Clinical Entity”, J Pediatrics and Child Health Issues, 3(4); DOI: http;//doi.org/03.2022/1.1047.
Copyright: © 2022 Manori Prasadani Thambiliyagodage. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly Cited.
Stridor with respiratory distress is an alarming clinical feature in the newborn, which warrants extensive evaluation and possible intervention depending on the etiology.
Bilateral vocal cord palsy is a relatively common etiology, apart from laryngomalacia, subglottic stenosis and congenital laryngeal webs. It may create a significant respiratory distress in the newborn compromising lung aeration, hence tissue oxygenation.
This case report discusses a rare cause of stridor in a newborn with lumbar meningomyelocele and hydrocephalus where an eventual diagnosis of Arnold- Chiari 2 malformation with bilateral vocal cord palsy was made.
Case Report
A term newborn was delivered in a tertiary care center in Sri Lanka, with an antenatal diagnosis of ventriculomegaly and lumbar meningomyelocele confirmed in the fetal anomaly scan. Immediately after birth the baby developed a significant stridor with respiratory distress. Examination revealed ruptured meningomyelocele (8*10 cm) with no cerebrospinal fluid leakage in the lumbosacral region. Both lower limbs were affected with bilateral talipes equinovarus. The baby was not dysmorphic. OFC- 32cm (50th centile) Both upper limbs were normal. Bladder was palpable at the umbilicus level, sacrum was normal, anus was patulous and urethral opening was normal.
As the baby was treated for neonatal sepsis and meconium aspiration, the initial respiratory distress was attributed to it.
Baby became ventilator dependent and weaning off to noninvasive ventilation failed repeatedly, requiring re-intubation all the time. several chest xays remained normal. Each time the baby was extubated significant stridor was encountered.
Following an ENT referral, baby underwent direct laryngoscopy twice. First one was inconclusive due to poor respiratory effort, second one confirmed bilateral vocal cord palsy. Meningomyelocele was repaired at the second week of life (Figure 2) and OFC was monitored closely. Baby’s OFC had a gradual increment of size up to 38 cm (95th centile) and the CT brain had, moderate lateral and third ventricle dilatation with marked colpocephaly, partial agenesis of corpus callosum and Arnold-Chiari 2 malformation. (Figure 3A & 3B)
Baby underwent an external ventricular drainage on day 48 of life and intracranial pressure was relieved. After this again a trial of extubation failed.
The reason for repeated extubation failures is the key learning point discussed in this case report. Finally, baby underwent tracheostomy on day 55 of life and was ventilator dependent. Figure 1.


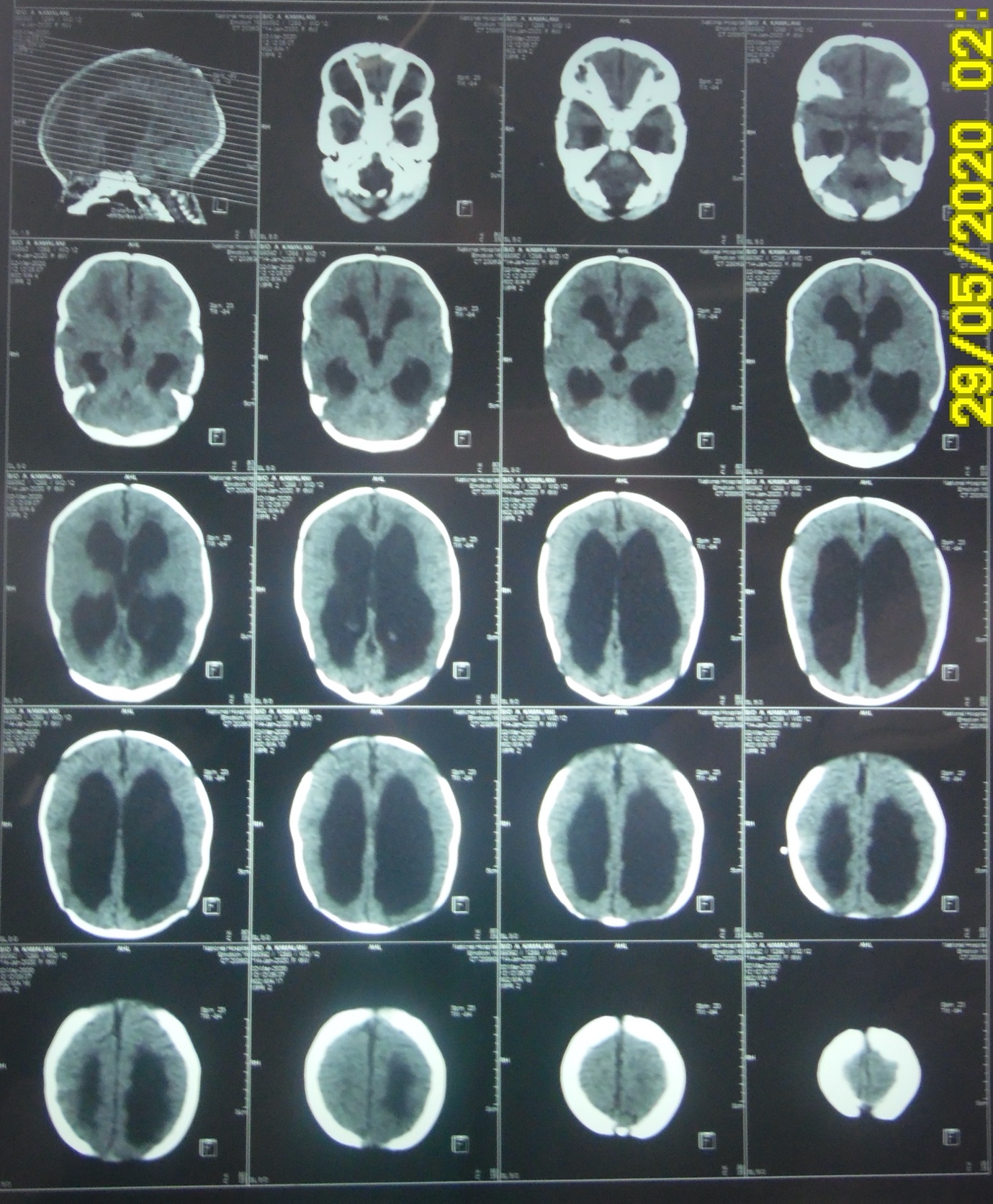
Figure: 3A Lateral and third ventricle dilatation, marked colpocephaly, partial agenesis of corpus callosum with Arnold-Chiari 2 malformation
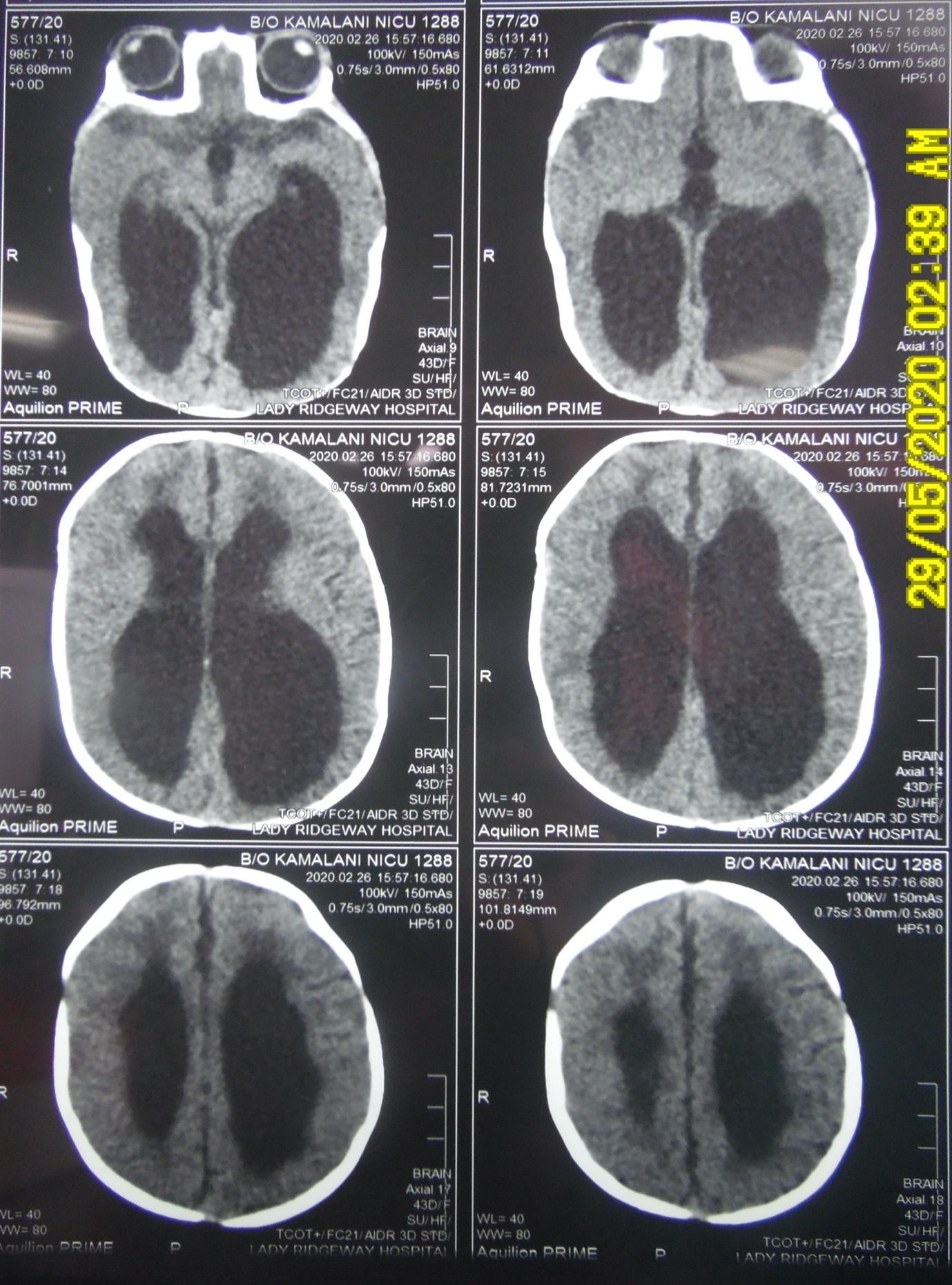
Figure 3B: Lateral and third ventricle dilatation, marked colpocephaly, partial agenesis of corpus callosum with Arnold-Chiari 2 malformation
Discussion
Bilateral vocal cord palsy is often idiopathic, but hold etiologies like Chiari 2 malformation, intraventricular hemorrhage, meningomyelocele, hydrocephalus which are neurological and traumatic forceps delivery, mediastinal surgery and ligation of patent ductus arteriosus as non-neurological cases (1)
Arnold-Chiari malformation is relatively a rare neurological condition with four subtypes. Type 2 is tonsillar displacement with lower medulla downward displacement and dysplasia of the medullary nuclei. It can be associated with lumbosacral meningomyelocele and aqueduct stenosis leading to hydrocephalus. It is well documented to be associated with bilateral vocal cord palsy (1)
Temporal association of vocal cord palsy with increased intracranial pressure is well described (1)
With the increased intracranial pressure there will be compression of vagus nerve, which is the nerve supply to cricoarytenoid muscle, responsible for vocal cord abduction (2,4,5)
Urgent ventriculoperitoneal shunts, external ventricular drainage, direct ventricular taps do have a place in immediate intracranial pressure release. Ideally it should be performed in first 48 hours of hind brain dysfunction (1)
Hind brain dysfunction will be evident by cranial nerve palsy, dysphagia, stridor and apnea. (1,4)
There will be an acute displacement of the malformed brain stem due to increased intracranial pressure, which needs immediate correction to equalize the intracranial and intraspinal compartment pressures. (1)
Delay in doing so will make the nucleus ambiguous degenerate, making the vocal cord palsy permanent (1,4)
This baby had a lot of other problems, which delayed release of the intracranial pressure and she ended up with a permanent tracheostomy and a respiratory support.
This case report highlights, the importance of considering vocal cord palsy in an Arnold- Chiari 2 malformation baby as a cause for stridor, and when repeated attempts of weaning off from ventilator fails.
This reflects upon early diagnosis and treatment to prevent complications.
Data availability:- not applicable
Conflicts of interest:- authors declare that there are no conflicts of interest.
Funding:- This study did not receive any funding in any form
Consent:- informed written consent is taken from both parents to publish the case with baby’s photographs.

Open Access By Aditum Open Access Journals id licensed under Creative Commons Attribution 4.0 International License. Based On a Work at aditum.org